Knee Joint Replacement
Unicondylar Knee Replacement (UKR) :: Total Knee Replacement (TKR)
Knee joint replacement helps patients in the treatment for severely diseased knee joints. A joint replacement procedure is designed to:
- Relieve pain
- Reduce symptoms
- Restore mobility
- Regain function
The knee joint can become worn-out most commonly as a result of osteoarthritis but may also result from other causes such as trauma or injuries, meniscal tears and overuse.
Joint Replacement Symptoms
Patients complain of the following symptoms
- Severe pain in the knee felt deep inside, the front, sides or back of the knee
- Swelling around the knee
- Sensation of ‘grating’ or ‘locking’ in the knee
- Pain at night
The pain is often made worse with walking or performing normal activities such as putting on shoes and socks, going up and down stairs or getting up from chairs,
Osteoarthritis Diagnosis
Dr. Brighton will need to diagnose the specific nature and extent of damage by osteoarthritis and which surgical approach will best serve you
Often, osteoarthritis can be identified during a physical exam by a medical professional. By examining the knee and leg bones the cause of symptoms can be pinpointed.
During this consultation Dr. Brighton will:
- Take a medical history
- Perform a physical examination
- Assess the joint’s range of motion
While there are is no blood test for osteoarthritis, other diagnostic methods are:
Imaging tests:
In order to clearly understand the nature of any loss of the joint space or bone spur formation imaging scans are required:
- X-rays do not show cartilage but normal films can help rule out other problems with the knee that may have similar symptoms like fractures (broken bone), loose bodies or ACL injury.
- MRI can create detailed images of both hard and soft tissues within your knee. An MRI can produce cross-sectional images of internal structures required if the diagnosis is unclear or if other soft tissue injuries are suspected such ligament injuries or articular cartilage injuries.
- Ultrasound - is rarely useful around the knee and certainly cannot help with the diagnosis of osteoarthritis
While not all of these tests are required to confirm the diagnosis, this diagnostic process will also allow Dr.Brighton to review any possible risks or existing conditions that could interfere with the surgery or its outcome.
Joint Replacement Surgery of the Knee
Knee replacement surgery is also referred to as knee arthroplasty.
During knee replacement, Dr. Brighton removes damaged bone and cartilage and can replace it with an artificial joint made of metal alloys, high-grade plastics and polymers.
There are three common approaches to damaged joints. Dr. Brighton offers:
- Knee cap replacement
- Partial joint replacement
- Total joint replacement
For each procedure, minimally invasive surgical techniques are applied and Dr. Brighton may also employ computer assisted technologies. This allows for optimised patient outcomes.
Knee Cap Replacement
Knee cap is also referred to as patellofemoral replacement arthroplasty.
This procedure is suitable for patients when arthritis only affects the knee cap and involves the replacement of the under-surface of the kneecap and its groove
The outcome of knee cap replacement can be good if the arthritis doesn’t progress and involves less procedural trauma offering speedier recovery times than a larger operation.
The results can be less predictable when compared to total knee replacement as arthritis can progress over time to other parts of the knee.
Some surgeons advise a total knee replacement as the results are more predictable, but that can be unnecessarily destructive if arthritis has not yet affected other areas.
The operation is only suitable for 2-3% of patients with osteoarthritis.
Unicondylar Knee Replacement (UKR)
Unicondylar knee replacement (UKR) or partial knee replacement simply means that only a part of the knee joint is replaced, and through a smaller incision than would normally be used for a total knee replacement.
Unicondylar knee replacements have been performed for decades and developments in implant design, instrumentation and surgical techniques have resulted in this approach being considered as the procedure of choice for unicompartmental arthritis.
Unicondylar Knee Replacement Approach
Your knee is divided into three major compartments:
- The medial compartment (i.e. the inside part of the knee)
- The lateral compartment (i.e. the outside part)
- The patellofemoral compartment (i.e. the front of the knee between the kneecap and thighbone)
In a unicondylar knee replacement, only the damaged compartment is resurfaced with metal and plastic. The healthy cartilage and bone in the remainder of the knee is left alone.
Advantages of Partial Knee Replacement
The benefits of a unicondylar knee replacement over a total knee replacement (TKR) are:
- The smaller incision
- Less bone removal
- Less blood loss
- Faster recovery
- Better range of movement
- A more “natural” feeling knee
Candidates for Partial Knee Replacement
Patients suitable for partial knee replacement are those who are:
- Suffering pain localised predominantly to a single area
- Have restricted mobility interfering with lifestyle
- Clinically proven to have only one diseased compartment (X-ray confirmed)
- Not suffering with severe angular deformity
- Not suffering inflammatory arthritis e.g. rheumatoid arthritis
- Not suffering an unstable knee
- Not previous osteotomy patients
- Not involved in heavy work or impact-loading sports
While a partial knee replacement can be considered at any age, the outcome of the surgery tends to depends on the extent of arthritis, rather than your age.
- Younger patients benefit from bone preservation which is helpful if you need revision surgery at a later stage
- Older patients would benefit from a less stressful operation with less pain and less risk of bleeding
Partial Knee Replacement Procedure
The procedure is designed to be performed with minimal local trauma
- A small incision around 8 cm is made to expose the knee joint
- The bone ends of the femur and tibia are prepared
- Components are then inserted to make sure they fit properly
- The final components are placed with or without cement
- The knee is then carefully closed and drains usually inserted
- The knee dressed and bandaged
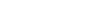
Total Knee Replacement (TKR)

A total knee replacement (TKR) or total knee arthroplasty is a surgery used to replace a knee joint that is affected by arthritis.
Total knee replacement surgery replaces the arthritic knee joint with an artificial metal or plastic replacement parts called the 'prostheses'. These include replacing the:
- End of the femur (thigh bone)
- End of the tibia (shin bone)
- Plastic inserted between them and
- Usually the patella (knee cap).
The artificial knee joint is made from a surgical-grade metal alloy with a special wear resistant plastic insert. Total knee replacement surgery is one of the most successful operations available today with over 90% still functioning well at 15 years.
Prior to surgery you will usually have tried some conservative treatments such as simple analgesics, weight loss, anti-inflammatory medications, modification of your activities, canes, or physical therapy.
Once these have failed it is time to consider surgery.
Candidates for Total Knee Replacement
The procedure is usually recommended for older patients who suffer from pain and loss of function from arthritis and have failed results of other conservative methods of therapy.
Each patient is assessed individually but total knee replacement candidature is far greater than partial knee replacement and can include candidates who are:
- Between 20 to over 80 years of age
- Suffering pain
- Having restricted mobility interfering with lifestyle
Total joint replacement can address patients with a greater range of arthritic stages and conditions.
Benefits of Total Knee Replacement Surgery
The decision to proceed with TKR surgery is a cooperative one between you, Dr. Brighton, family and other medical professionals.
The benefits following surgery are relief of symptoms of arthritis. These include
- Severe pain that limits your everyday activities including walking, shopping, visiting friends, getting in and out of chair, gardening, etc.
- Pain waking you at night
- Deformity- either bowleg or knock knees
- Stiffness
Components/Prostheses
The artificial knee joint consists of:
- An upper metal component shaped and sized to fit the femur bone contour
- A flat metal tibial component made of metal alloys fixed to the bone
- A plastic insert designed for low wear over many years
- A patellar button which resurfaces the back of your knee cap.
Total Knee Replacement Procedure
The procedure is designed to be performed with minimal local trauma
- Dr. Brighton cuts down to the bone to expose the bones of the knee joint.
- The damaged portions of the femur and tibia are then cut at the appropriate angles using specialised jigs.
- Trial components are then inserted to check the accuracy of these cuts and determine the thickness of plastic required to place in between these two components.
- The patella (knee cap) may be replaced/resurfaced depending on a number of factors and Dr. Brighton’s choice.
- The real components are then inserted with or without cement and the knee is again checked to make sure things are working properly.
- The knee is then carefully closed and the knee dressed and bandaged.
Each knee is individual and knee replacements take this into account by having different sizes for your knee. If there is more than the usual amount of bone loss, sometimes extra pieces of metal or bone are added.
Preparations Prior to Replacement Surgery
Once Dr. Brighton decides that surgery is required, preparation is necessary to achieve the best results and a quick and problem free recovery.
Preparing mentally and physically for surgery is an important step toward a successful result.
- Dr. Brighton will create a treatment plan and
- Patients will also need to understand the process and their role in it
Dr Brighton will also need to:
- Discuss any medications being taken with your doctor or physician to see which ones should be stopped before surgery
- Stop taking aspirin, warfarin, anti-inflammatory medications or drugs that increase the risk of bleeding one week before surgery to minimise bleeding
- Review blood replacement options (including banking blood) with your doctor
- Consider alternate medical interventions and other treatments
- Eat a well-balanced diet, supplemented by a daily multivitamin with iron.
- Consider losing weight (if overweight) before surgery to help decrease the stress on the new joint. However, dieting one month before surgery.
- Stop or cut down smoking to reduce your surgery risks and improve your recovery
- Treat any tooth, gum, bladder or bowel problems before surgery to reduce the risk of infection
Report any infections to Dr. Brighton prior to surgery as the procedure cannot be performed until all infections have cleared up.
Exercise Preparation
To help prepare you for the surgery a preoperative physiotherapist appointment is required to:
- Fit crutches (which should be brought to hospital)
- Instruction on weight-bearing and crutch usage
- Learning how to reduce inflammation (icing of the knees), and
- Learn postoperative exercise (co contractions, leg lifts with the knee extended, etc.).
Risks of Knee Surgery
As with any major operation, orthopaedic surgery has potential risks and complications. Surgical complications may include:
- Infection
- Stiffness of the knee
- Bleeding
- Blood clots
- Damage to local tissue
Dr. Brighton will discuss any concerns you may have before any procedure.
After Your Replacement Surgery
After your operation you will have a drip in your arm for pain medication and antibiotics.
You may need up to 5 nights in hospital. After that, you can choose to move back to your own home and continue physiotherapy as an outpatient or be admitted for Inpatient rehabilitation which is now widely available.
Crutches are required for 1 – 2 weeks following the replacement. It is usually a month before you have enough knee range and strength to drive.
If any postoperative problems arise with your knee, such as redness, increasing pain or fevers, do not hesitate to contact Dr. Brighton. If unavailable, seek advice from the hospital or your doctor.
Going Home after Replacement Surgery
Remember to arrange for someone to take you home, as driving is not usually recommended for a month.
Return to Work
You may return to light work duties after 2 weeks. You will not be fit to perform work duties that involve:
- Prolonged standing
- Heavy lifting
- Bending
- Excessive stair climbing
for a minimum of 4 – 6 weeks.
Postoperative Recovery Plan
Recovery from knee replacement surgery will usually take about 18 weeks.
The physiotherapist will prepare an exercise programme. Much of the exercise programme can be done at home or at a gym, under your physiotherapist’s guidance.
Strong analgesics will be required for at least the first 5-7 days including oral narcotics to manage the pain.
Strong pain killers (such as Panadeine Forte, Tramadol or Targin) are usually only required for the first 5-7 days. Thereafter, regular over-the-counter Panadeine should be enough to control the pain (especially at night).
Week 1:
- Ice your knee as directed by your physiotherapist
- Full extension (knee out straight) and gradually increasing flexion (bend)
- Full weight-bearing, wean off crutches
- Quads and hamstrings co-contractions
- Straight leg raises
- Ankle range of motion (ROM) exercises
If unsure about the exercise program after leaving hospital, a physiotherapist appointment will be required.
Week 2 – 6:
The first postoperative appointment with Dr. Brighton is needed 4-6 weeks following surgery. A postoperative knee X-Ray is required prior to this review appointment.
- Full weight-bearing – no limp – gait training
- Ice before and after exercise till swelling has dissipated.
- Isometric quad exercise
- Isokinetic closed chain exercises.
- Step work, leg press, squats
- Active knee flexion and extension
- Stationary bike
- Swimming – no restriction
- 21 days commence proprioception
Weeks 6 - 12:
Continuing strength and range of motion training.
After Week 12
Life gets pretty much back to normal with increasing activity. However, full recovery from knee surgery can be a slow process.
By 6 months:
- Recovery is normally fully completed
- Maximum range of motion has been regained
- Knee is usually strong enough to resume sports
- No analgesia is required